
The Low and High Serotonin Hypotheses of Depression
I recently had a deja vu in which I realized that life is hard. No one tells you that every day, every week, and every year new challenges rise up to kick you when you're down or to ruin your moment of celebration. Life is not all bad, but as students we can all remember, or are currently experiencing, times when we felt blue and down about exam scores or our future job prospects. Now I'm no doctor, but I would guess that during these moments when the gloom of reality weighs over your head like a dark cloud, your serotonin levels are low... or maybe high?A review published this January criticizes the age-old low serotonin hypothesis as the cause of depression. The authors instead claim that serotonin levels are high in patients with depression. Now I don't know about you but I love a MAVERICK who is willing to stand up against a long-standing hypothesis. Before I tell you more about this maverick, let me give you some background on depression. And of course, in this age of technology, I would be wrong not to provide you with a link to an online depression screening test, just in case you are worried your gloomy mood may be something more serious than just a reaction to a poor BIO 502 exam score. Click here.

Depression is the most
predominant illness among mental, neurological, and substance-use disorders (Owens and Nemeroff). It is also a common misconception to call depression a disease. Depression is really a mental disorder that consists of several different states. Symptoms include:
- Depressed mood or irritability most of the day
- Decreased interest or pleasure in most activities
- Significant weight change (5%) or change in appetite
- Change in sleep
- Change in sleep
- Change in activity
- Fatigue or loss of energy
- Guilt/worthlessness
- Diminished ability to think or concentrate, or more indecisiveness
- Thoughts of death or suicide (DSM IV)
This may seem like a lot of symptoms, some of which you may have experienced, but true depressive feelings do not go away and may present differently in every patient.
The leading hypothesis for the cause of depression is called the low serotonin hypothesis. It hypothesizes that the levels of serotonin, a neurotransmitter, fall below normal levels in the brain thereby inducing depressive symptoms. This hypothesis is the basis for the modern treatment of depression, the use of antidepressants. Serotonin is an important neurotransmitter for the hippocampus, the part of the brain involved in regulation of behavior, mood, memory, and learning (Strüder et. al.). The low serotonin hypothesis claims that the lowered levels of serotonin cause depressive symptoms. Basically, they think that the lack of a properly transferred serotonin signal leads to depressive symptoms. This happens when re-uptake of serotonin within the synapse lowers the levels of serotonin, decreasing serotonergic signaling(Owens and Nemeroff). Most scientists agree that serotonin has something to do with depression, however, the specific role of serotonin in depression is not fully understood.
How does serotonin work in the brain normally?
The basics: Tryptophan is the crucial precursor used to make serotonin. The main primary neurons that secrete serotonin are called serotonergic neurons, and are found in the dorsal raphe nucleus, which projects into the forebrain regions (Andrews, et. al.). Serotonin is transported into the presynaptic neuron by serotonin transporters. Once it is released and ingresses into the postsynaptic cell, it is degraded into 5-HIAA by mitochondrial enzymes (Andrews et. al.). The firing patterns of serotonergic neurons have different postsynaptic effects. For example, prolonged serotonin exposure can change postsynaptic firing from phasic to tonic. Serotonin is involved in almost all types of behaviors, including appetitive, emotional, motor, circadian rhythms, cognitive, and autonomic behaviors (Frazer and Hensler). In terms of physiology, is not clear whether serotonin affects behaviors specifically, or more generally by coordinating the activity of the nervous system (Frazer and Hensler).

The long story.... the activity levels of different parts of the brain change.
In a study comparing the brains of depressed and healthy people, researchers found that depressed patients had significantly increased activation of the anterior cingulate cortex, the insula, and the parahippocampal areas (i.e. the grey matter that surround the hippocampus) (Anand et. al.). The study concluded that depression is associated with increased activation of limbic regions, like the amygdala, pallido-striatum, medial thalamus, and insula (Anand et. al.).
 |
1: anterior
cingulate cortex; 2, 3: pallido-striatum; 4, 5: medial thalamus; 6, 7.
Are Current Treatments Really Treating?
There are two main treatments for depression: drugs (antidepressants) and electroconvulsive shock therapy (Owens and Nemeroff). I will focus on one specific drug therapy, selective serotonin re-uptake inhibitors or SSRI's. SSRI's "work" by blocking serotonin re-absorption into the cells that release it, keeping synaptic concentrations of the neurotransmitter high. This increases the responsiveness of the postsynaptic neuron in the hippocampus (Owens and Nemeroff), thereby alleviating symptoms. However SSRIs, and many other antidepressants, have a therapeutic delay, in that it takes several weeks for patients to see an improvement in depressive symptoms (Andrews et. al.). Andrews et. al. notes that SSRI's disrupt energy homeostasis. The reason for this is not well understood but Andrews et. al. argues that "it is the brain’s compensatory responses to SSRI treatment, rather than the direct pharmacological properties of SSRIs, that are responsible for reducing depressive symptoms" (Andrews et. al.). The authors hypothesize that the reason behind a reduction in serotonin levels is really a restoration of ENERGY homeostasis. This is because serotonin regulates the two major metabolic pathways for generating ATP from glucose. Serotonin affects electron transport in mitochondria and can upregulate or downregulate the production of ATP in the cytosol from glycolysis (Ashkenazy-Shahar and Beitner).
There are two main treatments for depression: drugs (antidepressants) and electroconvulsive shock therapy (Owens and Nemeroff). I will focus on one specific drug therapy, selective serotonin re-uptake inhibitors or SSRI's. SSRI's "work" by blocking serotonin re-absorption into the cells that release it, keeping synaptic concentrations of the neurotransmitter high. This increases the responsiveness of the postsynaptic neuron in the hippocampus (Owens and Nemeroff), thereby alleviating symptoms. However SSRIs, and many other antidepressants, have a therapeutic delay, in that it takes several weeks for patients to see an improvement in depressive symptoms (Andrews et. al.). Andrews et. al. notes that SSRI's disrupt energy homeostasis. The reason for this is not well understood but Andrews et. al. argues that "it is the brain’s compensatory responses to SSRI treatment, rather than the direct pharmacological properties of SSRIs, that are responsible for reducing depressive symptoms" (Andrews et. al.). The authors hypothesize that the reason behind a reduction in serotonin levels is really a restoration of ENERGY homeostasis. This is because serotonin regulates the two major metabolic pathways for generating ATP from glucose. Serotonin affects electron transport in mitochondria and can upregulate or downregulate the production of ATP in the cytosol from glycolysis (Ashkenazy-Shahar and Beitner).
The article challenges the low serotonin hypothesis and points out problems with the scientific data behind the hypothesis. These criticisms are summarized in BOX 1 to the left.
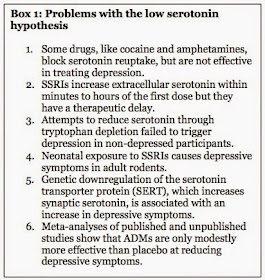 |
| Modified version of Box 1in Andrews et. al. |
Evidence shows that the initial worsening of symptoms occurs when the largest increases in extracellular serotonin occur (Andrews et. al.). It is only over several weeks of treatment that depressive symptoms reduce, during which the trajectory of extracellular serotonin is declining. The authors suggest that decreasing serotonin levels in limbic regions is important for the therapeutic effect of antidepressants.
 |
| Figure 4 from Andrews et. al. Fluox is fluoxetine, a common SSRI |
Fig.3. Hypothetical serotonin and glutamate patterns over the course of depression and SSRI treatment.
|
References:
Anand, A., Y. Li, Y.
Wang, J. Wu, S. Gao, L. Bukhari, V.P. Mathews, A. Kalnin, and M.J. Lowe. 2005.
Activity and connectivity of brain mood regulating circuit in depression: a
functional magnetic resonance study. Neuropsychopharmacology 30:1334–1344.
Andrews, P.W., A.
Bharwani, K.R. Lee, M. Fox, and J.A. Thomson Jr. 2015. Is serotonin an upper or
a downer? The evolution of the serotonergic system and its role in depression
and the antidepressant response. The Journal of Neuroscience and Biobehavioral
Reviews 51:164–188.
Ashkenazy-Shahar, M., and
R. Beitner. 1997. Serotonin decreases cytoskeletal and cytosolic glycolytic
enzymes and the levels of ATP and glucose 1,6-bisphosphate in skin, which is
prevented by the calmodulin antagonists thioridazine and clotrimazole. The
Journal of Biochemical and Molecular Medicine 60:187-193.
DSM-IV. Diagnostic Criteria for Major Depressive Disorder and Depressive Episodes. http://www.psnpaloalto.com/wp/wp-content/uploads/2010/12/Depression-Diagnostic-Criteria-and-Severity-Rating.pdf
Frazer, A. and J.G. Hensler. 1999. Serotonin Involvement in Physiological Function and Behavior. Basic Neurochemistry: Molecular, Cellular and Medical Aspects. 6th edition.
Frazer, A. and J.G. Hensler. 1999. Serotonin Involvement in Physiological Function and Behavior. Basic Neurochemistry: Molecular, Cellular and Medical Aspects. 6th edition.
Owens, M.J., and C.B.
Nemeroff. 1994. Role of serotonin in the pathophysiology of depression: focus
on the serotonin transporter. The Journal of Clinical Chemistry 40:288-295.
Strüder, H.K., and H.
Weicker. 2001. Physiology and Pathophysiology of the Serotonergic System and
its Implications on Mental and Physical Performance. Part I. International
Journal of Sports Medicine 22:467-481.
Winokur, A., K.A Gary, S.
Rodner, C. Rae-Red, A.T. Fernando, and M.P. Szuba. 2001. Depression, sleep
physiology, and antidepressant drugs. Journal of Depression and Anxiety
14:19-28.