Michael Wade
About a week ago, one of my friends posted a video on
Facebook that started a big debate and lead to this post. In the video, this
guy was advertising Kangen water and it’s filtration system. The guy wasn’t
scientifically literate, saying things incorrectly about chemistry and biology
that he should have learned in high school. The claim that I got in a debate
about was that drinking alkaline water is good for you because it’s literally
putting millions and millions of electrons into your body to fight off oxidation.
Made me laugh. I told my friend to drink lye (NaOH), find a literature article
to support the claims and get back to me. Well… he didn’t drink lye, but he did
give me some literature, which prompted my interest in this subject, and will
hopefully get some wheels turning in your heads too.
The terms electrochemically and naturally reduced waters are
probably foreign to many people. Electrochemically reduced water (ERW) is electrolyzed
water produced near the cathode, usually platinum coated, during electrolysis
and tends to be alkaline, with a pH of 8-10 (Fig.1). ERW are high in H2
gas and is hydrogen molecule-rich. Naturally
reduced water (NRW) is water that naturally has high levels of H2
gas and is hydrogen molecule-rich. NRW reserves have been found in some parts
of Japan and Mexico.
 Figure 1. Preparation of electrolyzed water (A), and
Chemical reactions at the surface of the platinum cathode (B). (Shirahata et al.2011)
Figure 1. Preparation of electrolyzed water (A), and
Chemical reactions at the surface of the platinum cathode (B). (Shirahata et al.2011)
A lot of research is going on in Japan on the benefits of
ERWs and NRWs. Much of the research is focusing on diabetes, but there are many
other disease models being investigated including uses as an anti-neurodegenerative
and anti-cancer drug. This blog will focus mainly on the effects of reduced
water and diabetes both in vitro and in vivo.
Type 1-diabetes is a chronic lifelong disease characterized
by too much glucose in the blood caused by damaged or nonfunctional b cells. In mouse models,
diabetes can be induced with certain drugs whose meachanism is not fully
understood, but acts through the production of reactive oxygen species and
selectively targest pancreatic b
cells. Li et al. induced Type
1-diabetes in a hamster cell line with the diabetogenic drug alloxan. The b pancreatic cells were
incubated with different waters prior to exposure to alloxan, then tested for
viability. The ERWs and NRWs showed an increase in viability compared to the
control after exposure to alloxan(ultra pure water) (Fig.2). Since alloxan
increases ROS in b cells, it is believed that these ERWs and
NRWs (from here on will be refered to as RW) exhibit their protective effect
via their ability to scavenge and neutralize ROS, which is supported by
previous studies showing an antioxidant effect of RWs. Glucose induced insulin
secretion was also increased in RW treated groups. Li, et al. hypothesized that this is due to an increase in glucose
sensitivity because RW did not increase insulin secretion without glucose
stimulation.
As we all know, success with in vitro experiments doesn’t mean success with in vivo experiments. However, with the case of diabetes and RW, in vivo animal models are working and
clinical trials are currently being performed. In genetically diabetic mice (db/db), Kim et al. showed that RW significantly lowered the blood glucose
levels and raised the insulin levels. In the db/db mice, the size of the pancreas was significantly smaller than
that of the control, and interestingly enough, RW treatment increased the size
of the pancreas, which is probably why the insulin levels increased.
Type 2-diabetes mice models are also showing success. Jin et al. show that OLETF (type 2-diabetic
mice) that blood glucose levels are consistently lower than control mice. One
characteristic of type 2-diabetes is hyperlipidemia. OLETF mice treated with RW
had significantly lower levels of cholesterol and triglycerides in the blood.
Not only do RWs protect against diabetes, but they also protect against
diabetic-related complications such as heart disease. GOT and GPT are amino
transferases that are secreted into the blood from damaged heart cells. This
damage has been linked to lipid deposition the coronary artery causing a
blockage, leading to oxygen deficiency. In RW treated mice, the concentration
of secreted GOT and GPT were lower than those in the control which is expected
due to lower blood lipid levels.
Figure 2. Effect of Tap water vs. RW in Type 2 diabetic mice
after an intraperitoneal injection of glucose. (Shirahata et al.2010)
Although the exact mechanism of how RWs treat diabetes, Shirahata
et al. have started to fill in some
gaps in the insulin cascade. RWs promote phosphorylation of the B-subunit of
the insulin receptor via suppression of redox-sensitive tyrosine phosphatases.
RWs also activate Akt, a PI3 kinase, which is required for translocation of the
glucose transporter, GLUT4, to the plasma membrane. Akt also plays a role in
lipid metabolism; however, nobody has looked specifically at that mechanism due
to a greater interest in glucose metabolism.
In Japan, there have been a few clinical studies that have
shown promise for diabetic patients. An a study with 411 type 2-diabetes, 45%
of patients who drank RW showed significantly lower levels of blood glucose,
blood cholesterol, LDL (bad cholesterol) and creatine and higher HDL 6 days. A
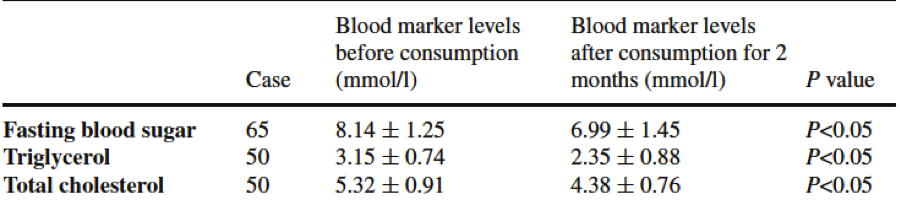
similar study of 50 patients over a two month period showed 89% of patients had
a significant decrease in blood glucose, 92% showed a significant decrease in
blood triglycerides and total cholesterol levels. Although these two studies
weren’t double blind, two double blind studies were conducted later and showed
very similar results.
Table 1. Suppressive
effects of RW on 65 diabetic patients and 50 hyperlipidemia patients.
(Shirahata et al.2010)

Patients in end-stage renal disease suffer T-cell damage
caused by oxidative stress, leading to T-cell apoptosis; patients also have and
a low cytokine level and the ratio of Th1/Th2 is not normal. Due to its
antioxidant properties, RWs were investigated as a possible treatment in 42
end-stage renal disease patients compared to 12 healthy individuals. After one
year of RW treatment, there was a significant increase in the amount of
T-cells, a significant decrease in T-cell apoptosis, and the intracellular
levels of cytokines was significantly increased, and the ratio of Th1/Th2 was
returned to normal levels.
Figure 3. Variety of functions of RW. (Shirahata et al.2011)
On one last note, if diabetes treatment didn’t keep your
interest, then maybe this will. RWs have been shown to reduce ethanol-induced
hangovers in mice by significantly increasing alcohol dehydrogenase and
acetaldehyde dehydrogenase in liver tissues. Although I don’t know of any
clinical trials for this, there probably would not be a shortage of volunteers
in the college community who wouldn’t want to test this...
RWs are showing great therapeutic potential in a variety of
diseases. One of the hallmarks of RWs is that it is completely safe and has
zero side effects. Since this “miracle water” has been shown to act as a
therapeutic agent for many diseases in Japan, it makes you wonder why there’s
almost no research on it here in America. Part of me can’t help but think that
the big pharma doesn’t want to make this research known because of the profits
they make from disease…
References:
Park, S., Qi, X., Song, S. et al. Electrolyzed-reduced water
inhibits acute ethanol-induced hangovers in Sprague-Dawley rats. 2009.
Biomedical research. 30(5): 263-269.
Shirahata, S. Hamaski, T., and Kiichiro Teruya. Advanced
research ofn the health benefit of reduced water. 2011. Trends in Food Science
& Technology. 23: 124-131.
Li, Y., Nishimura, T., Teruya, K., et al. Protective
mechanism of reduced water against alloxan-induced pancreatic b cell damage: Scavenging
effect against reactive oxygen species. 2002. Cytotechnology. 40: 139-149.
Nakayama, M., Nakano, H., Hamada, H., et al. A novel
bioactive haemodialysis system using dissolved dihydrogen (H2)
produced by water electrolysis: a clinical trial. 2012. Nephrology Dialysis
Transplantation. 25:3026-3033.
Kim, M., Jung, K.H., Uhm., Y.K., et al. Preservative effect
of electrolyzed reduced water on pancreatic b
cell mass in diabetic db/db mice.
2007. Biological and Pharmaceutical Bulletin. 30(2): 234-236.
Jin, D., Ryu, S.H., Kim, H. W., et al. Anti-diabetic effect
of alkaline reduced water on OLETF rats. 2006. Bioscience Biotechnology and
Biochemistry. 70(1): 31-37.
Huang, K., Hsu, S., Yang, C., et al. Electrolysed-reduced
water dialysate improves T-cell damage in end-stage renal disease patients with
chronic haemodialysis. Nephrology Dialysis Transplantation. 25: 2730-2737.














){kind=link}