Growing up with asthma my symptoms would flare up and I
would end up bedridden, coughing, and wheezing all day. Yet as I waited in the
patient room of my pediatrician's office, I began feeling better before the doctor
examined me. The medication he prescribed reduced inflammation and relaxed the
muscles of the airways, which physiologically aided my breathing. However, my expectations influenced why I
began feeling better prior to medical treatment. There are numerous
studies on various ailments where patients treated with inert medications
resulted in feeling better. These inert substances in the form of pills,
creams, and "sham treatments" are known as placebos.

Background on the Placebo
Placebo is derived from the Latin word”placer” which
means "to please" rather than to benefit (Sonawalla; Finniss et al).
It has been defined as a form of medical therapy intervention to provide a
psychological effect and also include medical therapies not efficacious that
were thought to be at the time. In addition, placebos have also been used to
eliminate observer bias in experimental settings.
Factors such as the attitude of the physician, patient suggestibility,
and type of treatment can all influence the effects of placebos. Other factors involve
the natural course of the disease, or biological variation in
the individual. The placebo response is an apparent improvement in
the clinical condition of the patient. Although placebos provide beneficial
effects, they can also induce “adverse effects” when patients are previously
warned of the drug side effects (Sonawalla).
Placebo Response to Pain
Placebo analgesia is the most understood type of placebo response,
dating back to WWII when there was no informed consent. One of the founders
investigating the effects of the placebo was Henry Beecher, an army doctor in
the 1950's, who faced the problem of not having enough morphine during
battlefield and told his patients he was administering morphine when it was saline,
which does not have analgesic properties (Benedetti). Interestingly, 40% of his patients claimed to
experience a reduction in pain from saline treatment.
 |
| Henry Beecher attending a wounded American Soldier during WWII |
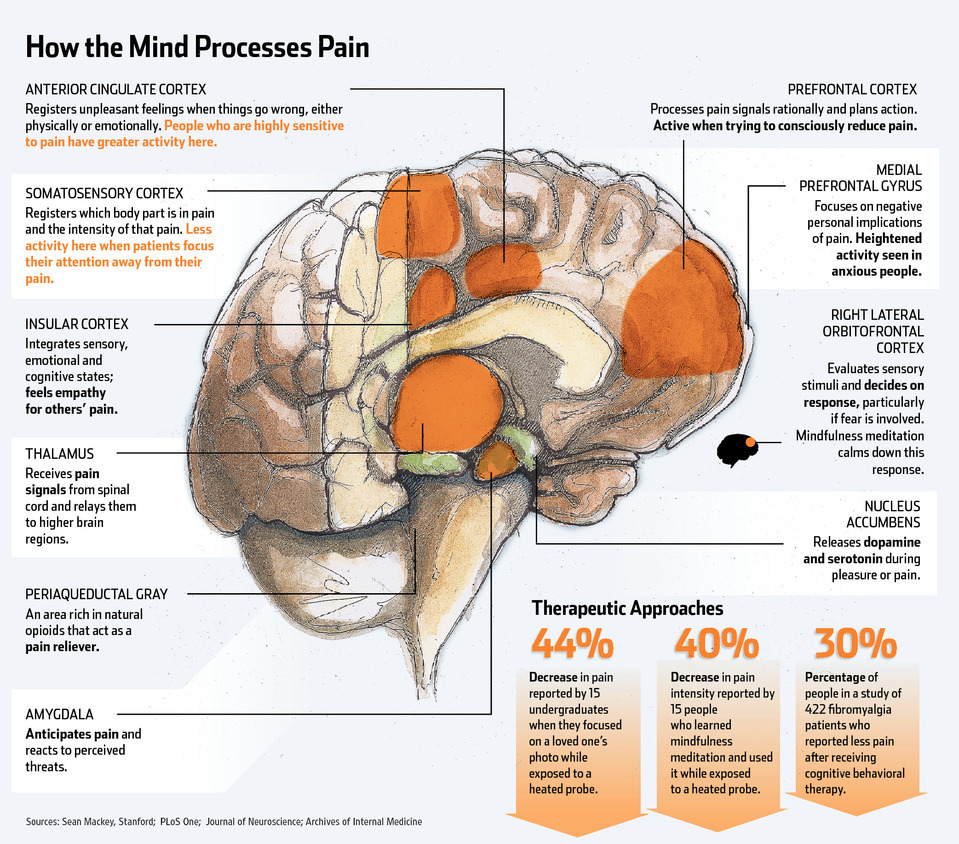
Areas in the Brain that are Affected
 |
| Various location in the brain process pain stimulation |
 |
| Benedetti 2013 |
The first image depicts areas in the brain that
process different types of pain. The second figure illustrates a meta-analysis of
the active areas in the brain, represented in red, during stages of
anticipation of analgesic after pain stimulation (top panel). These areas
include the anterior cingulate, medial and lateral prefrontal cortices,
thalamus, and hypothalamus (middle panel). Deactivations of pain activity are indicated
in green (bottom panel) following the administration of placebo analgesia
(Benedetti). Meta analysis is a combination of results from previous studies to
compare and contrast statistical data.
Here is a short video on how endogenous opioids throughout
the brain and spinal cord modulate incoming pain information. Although the
jargon is technical, the overall message explains that the body produces
endogenous opiates through electrical stimulation of the central nervous
system.
Drug opiates such as morphine and heroine are highly
effective, yet addictive. Endogenous opiates formed within the body also appear
to provide similar functions when placebo is administered in some patients. The
neurobiology of placebo was discovered when an opioid antagonist, naloxone,
inhibited the placebo analgesic response (Amanzio and Benedetti). The two predominating hypotheses for the
placebo response are the conditioned association between active analgesic and
pain relief and the reduction in anxiety resulting from the expectation of
relief.
Comparison of Two Placebos to Reduce Pain
The placebo effect serves as a model to understand the
endogenous mechanisms of analgesia, especially since studies show that placebos
activate different endogenous antinociceptive systems (Benedetti). One study
compared two different placebos on 270 patients with chronic arm pain. Patients
who underwent 6 weeks on "sham acupuncture" treatment had a
significant reduction in pain compared to the placebo pill group (P < 0.001)
(Kaptchuk et al).

The "sham acupuncture" used needles that did not
actually penetrate the skin of the patients; meanwhile the pills administered
were made out of cornstarch. Compared to baseline pain category (phase 1),
patients in both groups experienced decreases in
pain (phase 2).
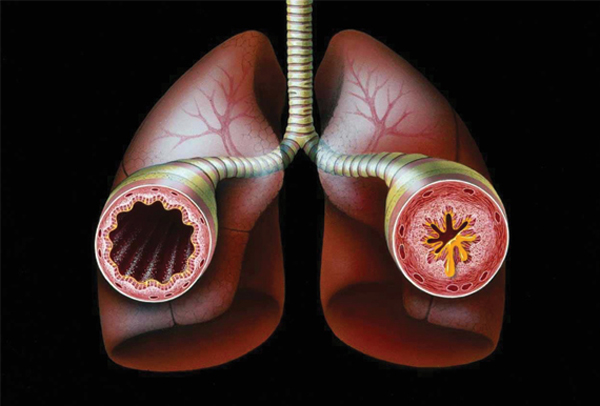
Placebo Response in Asthma
 |
| The airway on the right lung is normal while the left airway is a representation of a patient with Asthma symptoms. |
Moreover, a placebo
effects study was conducted on asthma patients in which four treatment groups
were compared: active albuterol inhalers, placebo inhalers, sham acupuncture,
and no treatment.


Physiologically, airway obstruction is measured by force
expiratory volume in 1second (FEV1) which is measured when a patient blows onto
a force expiratory maneuver. The results
from the graph show that the albuterol inhalers demonstrated a significant percent
change in FEV1 (P < 0.001) compared to the other three groups (Wechsler et
al).
Yet the percent change in subjective improvement for each
group based on a visual analogue scale 1-10 was surprising. Patients
significantly claimed to feel better in the albuterol group 50%, sham
acupuncture 46%, and placebo inhaler group 45% compared to the control (P < 0.001). Even though the placebos had no physiological effects in
patients via improved airways, they perceived a reduction of their symptoms. The
percentage of patients in active albuterol claiming to feel better was not
significantly different to the response in patients in the two other placebo
groups.
Ethical Issues with Placebos
Although I am not advocating the use of placebos in medicine, I was intrigued about the studies conducted in the field, and learned some interesting things in the process. Ted Kaptchuk, a renowned researcher in the field of placebos at Harvard Medical School, grew an interest in his study as he witnessed some patients claim to feel better before their treatment began. His value of acupuncture was not obscured, which led him to suspect that there were other contributing factors (Feinberg). Many argue that placebos can be dangerous because they do not physiologically reduce the natural course of the disease, but simply reduce the perceived symptoms of the patients. Critics argue that patients may not seek actual medical treatment when they are set to believe that they are better when in reality, they are not.
Although I am not advocating the use of placebos in medicine, I was intrigued about the studies conducted in the field, and learned some interesting things in the process. Ted Kaptchuk, a renowned researcher in the field of placebos at Harvard Medical School, grew an interest in his study as he witnessed some patients claim to feel better before their treatment began. His value of acupuncture was not obscured, which led him to suspect that there were other contributing factors (Feinberg). Many argue that placebos can be dangerous because they do not physiologically reduce the natural course of the disease, but simply reduce the perceived symptoms of the patients. Critics argue that patients may not seek actual medical treatment when they are set to believe that they are better when in reality, they are not.
Yet valuable outcomes of placebo studies are that they
highlight multiple factors involving self-improvement which could provide a
better understanding of doctor-patient interaction. Although placebos studies
still require much more research before we can understand their use for medical
treatment, we can infer that placebos aid in the understanding of the mechanism
of drug action from the effects of suggestion, as well as for eliminating bias
on the patient and observer part in clinical trials (Beecher).
Citations
Amanzio, M., & Benedetti, F. (1999).
Neuropharmacological dissection of placebo analgesia: expectation-activated
opioid systems versus conditioning-activated specific subsystems. The
Journal of Neuroscience, 19(1), 484-494.
Beecher, H. K. (1955). The powerful placebo. Journal of the
American Medical Association, 159(17), 1602-1606.
Benedetti, F. (2013). Placebo and the new physiology of the
doctor-patient relationship. Physiological reviews, 93(3), 1207-1246.
Feinberg, C. (2013). The placebo phenomenon. Harvard
Magazine, 36-39.
Finniss, D. G., Kaptchuk, T. J., Miller, F., & Benedetti,
F. (2010). Biological, clinical, and ethical advances of placebo
effects. The Lancet, 375(9715), 686-695.
Kaptchuk, T. J., Stason, W. B., Davis, R. B., Legedza, A.
R., Schnyer, R. N., Kerr, C. E., ... & Goldman, R. H. (2006). Sham device v
inert pill: randomized controlled trial of two placebo treatments. British
Medical Journal, 332(7538), 391-397.
Sonawalla, S. B., & Rosenbaum, J. F. (2002). Placebo
response in depression. Dialogues in clinical neuroscience, 4(1), 105.
Wechsler, M. E., Kelley, J. M., Boyd, I. O., Dutile, S.,
Marigowda, G., Kirsch, I..& Kaptchuk, T. J. (2011). Active albuterol or
placebo, sham acupuncture, or no intervention in asthma. New England Journal of
Medicine, 365(2), 119-126.
Image sources (in order of appearance)
{kind=link}
{kind=link}
Figure 8 (Benedetti, 2013).
https://www.youtube.com/watch?v=FbJF8gijf8E
Figure 2(Kaptchuk 2006)
{kind=link}
Figure 3 (Wechsler et al 2011)
Figure 4 (Wechsler et
al 2011)